Some readers have left comments saying that beauty lies in the eye of the beholder. Information addressing this issue has been scattered over multiple pages, but instead of linking to these pages everytime someone raises this issue, it is best to come up with a single page where a brief summary with links to the details is presented. This entry will also be addressing some topics that have not been addressed previously.
How does one go about showing that there are objective correlates of beauty?
This is easy to answer. One should show universal agreement and provide evidence that these correlates have some biological significance other than merely helping attract more potential mates and/or show that these correlates are sufficiently abstract in order to render implausible the notion that universal or broad agreement as to what constitutes beauty does not merely reflect social conditioning.
There are numerous correlates of beauty. It is common observation that people do not unanimously agree about the minutiae of what constitutes beauty. However, some people have defective eyesight/vision and/or a variety of brain abnormalities. Therefore, universal agreement cannot be expected, but one should still consider whether there is broad agreement and how mentally normal are those who deviate from the broad agreement.
Here are some objective correlates of beauty addressed within this site so far, where objective is understood as broad agreement in the population:
- People strongly and overwhelmingly aesthetically prefer above average femininity in the looks of women.
- The page linked to in point #1 addresses other objective correlates of beauty such as averageness and fluctuating asymmetry.
- A page addressing aesthetics in international beauty pageants discusses the components of beauty mentioned in #1 and #2 above in the context of correlates that cannot be explained in terms of social conditioning because they are either sufficiently abstract or are known to have biological significance other than merely helping attract more potential mates, as in above average femininity in women corresponding to higher fertility and fecundity. This page also addresses whether pedomorphy is a correlate of beauty and the correlate of beauty concerned with placement of face shape along the overall ancestral-to-derived discriminant.
- Most people in Western culture find neither skinniness nor obesity socially acceptable.
- Most men and most women judge the attractiveness of women similarly; this has been reported for evaluation of facial attractiveness (see #1 above), waist-hip proportions and physique.
Masculinity-femininity and attractiveness in women
The major correlate of beauty that this site is focusing on is masculinity-femininity as it pertains to attractiveness in women. Given that the general public overwhelmingly and strongly aesthetically prefers above average femininity in the looks of women, one could ask whether this is a normal preference.
For starters, between men and women, it hardly needs to be mentioned which group is supposed to look feminine by design. It is also the case that more feminine women also tend to be more fecund and fertile. Therefore, the majority preference, i.e., a preference for feminine looks in women, appears to be normal -- as in resulting from design -- and an aesthetic preference for masculinized women appears anomalous. This suggestion should be assessed in light of the characteristics of people who prefer masculinized looks in women. Masculine looks in women are disproportionately preferred by homosexual/bisexual men, lesbian/bisexual women, women with gender identity disorder, anorexics, bulimics and masculinized women (anorexic and bulimic women tend to be more masculine than normal women, on average; see evidence from sex hormone profiles).
Gender identity disorder, anorexia and bulimia are bona fide mental disorders. Based on random, population-based sampling, it has also been shown that nonheterosexuals have a 2-3 fold higher prevalence of mood disorders, anxiety disorders and substance use disorders compared to exclusively heterosexual individuals, which is largely unaccounted for in terms of stigma, prejudice, victimization and discrimination, and is basically intrinsic to nonheterosexuality. Therefore, a preference for masculinized looks in women has an association with mental abnormality. Now, it would be a stretch to expect every single incidence of a preference for somewhat masculinized women on the part of exclusively heterosexual men as abnormal since there is a possibility that a man could produce a more masculine son than himself by reproducing with a somewhat masculinized woman. Therefore, whereas every single incidence of a preference for masculinized features in women cannot be called abnormal, given the association of the latter with mental abnormality and its statistical atypicality, this preference is appropriately designated anomalous and is abnormal in a number of cases.
It also needs to be pointed out that a number of masculinized women appear to go through an agonizing period in youth where they are not comfortable with their masculine looks, but eventually learn to live with it and may even end up regarding soft and feminine features as less desirable (a case of sour grapes as in the classic Aesop’s fable of The Fox and the Grapes).
Cultural differences and beauty
Some may attempt to point out examples shown in Table 1 to argue for cultural determinants of beauty/good looks and therefore the historical and geographical arbitrariness of beauty standards.
| Table 1. Some forms of body adornment/modification; click images for larger versions. | |
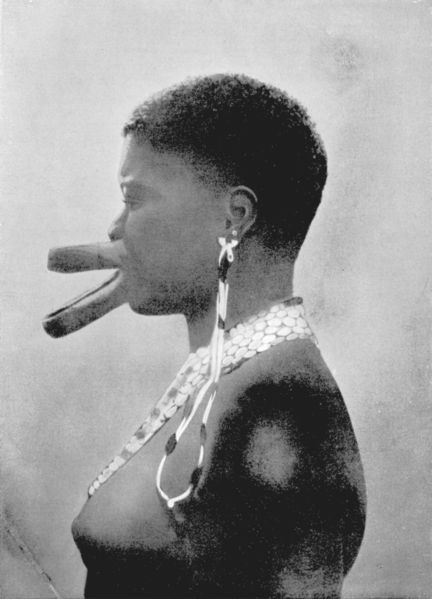 |
Sara woman with lip plates |
 |
Padaung woman with neck rings |
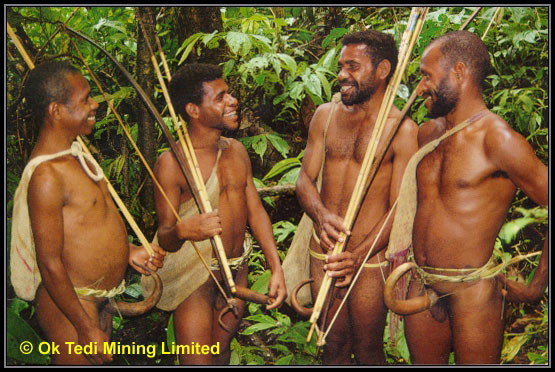 |
New Guineans with penis sheath |
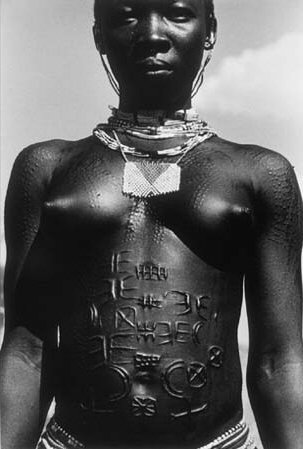 |
Nuba woman with scarification |
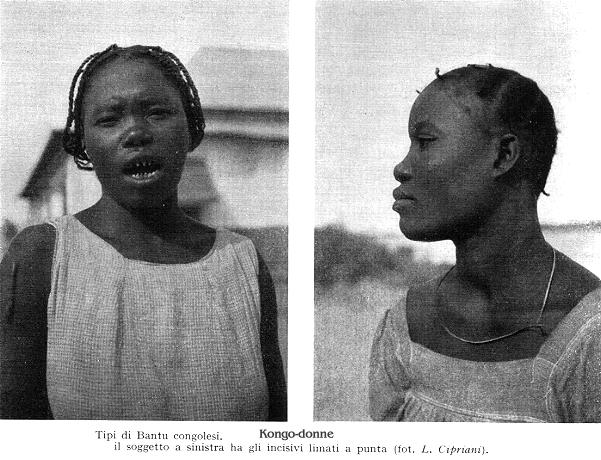 |
Congolese with filed teeth |
 |
Native American with skull deformation resulting from head binding |
 |
North American punk |
 |
Pierced and tattooed North American lesbian |
 |
Dani warrior |
Do the examples shown in Table 1 justify the arbitrariness accusation? Think again. Body adornment/modification/fashion wear should be distinguished from appreciation of the body as it comes. In contemporary Western culture, fashionable wear that was in vogue two decades ago may be a fashion faux pas today, but a general public preference for above average femininity in the looks of women has remained, notwithstanding the gay domination of the fashion business leading to masculinized women ending up being the most well-recognized/top models.
Shamans are the holy men in hunter-gatherer societies, and are disproportionately psychotic. A deranged and influential shaman could lead his followers to adopt and pass down a variety of bizarre practices. In the beginning, reluctant individuals could be initiated into a weird practice upon fear of divine retribution/possession by demons, but later it would simply become tradition/initiation rite that people have to comply with if they are to remain members of the tribe/prove tribal allegiance, wherein some form of pain would come in handy to break down an individual and make him part of the group, ready to fight for the tribe if needed. People could even come to appreciate a bizarre form of body modification because it supposedly keeps evil spirits away or something equivalent. The variability of the practices adopted can be assumed to reflect the variability of the specifics of the mental illnesses of the shaman founding fathers of the cultures, but the general theme -- i.e., schizophrenic powerful shamans founding bizarre behaviors -- would hold across cultures.
One type of mental illness among shamans is of special note when it comes to the establishment of body modification practices involving pain, namely sadomasochism, wherein sadism refers to deriving pleasure from delivering pain unto others and masochism refers to deriving pleasure from being subjected to pain; such pleasure may be of a sexual nature. Western individuals into sadomasochism are disproportionately found with piercings and tattoos.
Note also that some practices -- such as wearing a penis sheath or elongating the female neck -- serve to exaggerate sexual dimorphism. In other words, there is a common underlying principle but different forms in which it manifests itself.
In short, it is not all arbitrary. There are common underlying principles behind body modification across cultures though there is variation when it comes to the specifics.
The issue of obesity
Some cultures -- disproportionately in sub-Saharan Africa, the Middle East and also in Asia -- value excess body fat in women, whereas obesity is not considered socially acceptable in Western culture. Arbitrary cultural difference? Not so fast.
Body fat can come in handy during food shortages. In humans and apes, the best place to store body fat for rapid and easy mobilization upon need is the abdomen. Genes that allow one to store considerable body fat if plenty of food is available and one can get by with minimal physical labor may be advantageous in some situations.(1) Numerous such thrifty genes have been identified. Since body weight is typically well regulated, those without such thrifty genes, even if eating ad libitum and engaging in minimal physical labor, will typically not gain body fat in adulthood (after removing the influence of aging-related degenerative changes).
In a population where many people do not have enough to eat and many engage in heavy physical labor, a preference for overweight/obesity may exist if the prevalence of thrifty genes in this population is high. This can be expected because many high status individuals in such a population will posses thrifty genes and most likely end up obese given plenty of food and reduced need for physical labor on their part. Additionally, in such a population, if the unreliability of food supply and/or an undeveloped societal state necessitating heavy physical labor on the part of most individuals persists for a long time, then one can expect that the genetics associated with aesthetic tolerance of overweight/obesity or, in some cases, even a preference for obesity will be widespread. Whereas obesity results in negative health consequences, given that high status confers numerous social benefits, if the acquisition of some physical traits associated with high status results in delayed adverse health consequences, which is the case with obesity, then several individuals can be expected to direct their behavior toward the acquisition of physical traits associated with high status.
Back to thrifty genes, let us address the 825T allele of a gene that encodes for a G-protein beta-3 subunit.(2-4) Across different human populations, those having two copies of 825T are two- to three-fold more likely to be obese compared to those having two copies of 825C (the ancestral allele).(3) G-protein activation appears to be a thrifty genotype that facilitates body fat storage; the 825T allele predicts enhanced activation.(2-4) The frequency of the 825T allele varies as follows: sub-Saharan Africans (74-91%), African-Americans (72%), Australian Aborigines (72%), !Kung (66%), New Guineans (50%), Arabs (45-56%), East Asians 42-52%), American Indians (11-42%), and Europeans (21-35%).(3)
Consistent with the above, if plenty of food and reduced need for physical labor are available, such as in the West, the prevalence of obesity is much higher among African-Americans(5, 6) and Australian Aborigines(7) compared to whites.
Among American white women, the prevalence of obesity decreases with increasing socioeconomic status (SES), but the prevalence of obesity across socioeconomic classes remains roughly constant for African-American women.(8) The decrease in obesity with increasing SES is a robust find among white women everywhere. In developing nations, the prevalence of obesity among women increases with SES,(9) and the reason a similar relationship is not seen among African-American women is because they have plenty to eat across all socioeconomic classes. Among American white men, there appears a trend wherein the prevalence of overall obesity is somewhat lower at the extremes of SES, whereas the prevalence of obesity increases with SES among African-American men,(8) which is consistent with the far greater acceptance of obesity among African-Americans compared to American whites.(10)
The 825T allele is not the only genetic factor implicated in obesity, but the point should be clear. In a population where few of the socioeconomic elite have a tendency to become obese, a societal preference for obesity/social acceptance of obesity is unlikely to arise since one would not be seeing a lot of obese upper class people. An example of such people are the Scandinavians and the Dutch. The Scandinavians and the Dutch have a low tendency toward obesity, and among them there is a sharp socioeconomic gradient in the prevalence of obesity(11-14) that is not explained by educational and lifestyle factors.(11, 14, 15) One can assume that the socioeconomic gradient is largely explained by genetic factors. In short, population differences in the social acceptability of obesity should not be assumed to result from arbitrary cultural differences, and the contribution of genetic differences should be considered.
Conclusions
There are individual and cultural differences with respect to what one finds physically attractive, but these differences do not undermine broad agreement about what constitutes beauty. Some cultural/sub-cultural differences are almost certainly a result of genetic differences or mental illnesses, whereas some individual differences in aesthetic preferences are part of normal variation.
The statement that beauty lies in the eye of the beholder is misleading. Whereas it is typically true that whatever one’s physical appearance, there will be some people who will find one attractive, some people are found to be attractive by many or most people whereas others are found unattractive by many or most people, which is not readily explicable in terms of social conditioning. Therefore, when women seen in beauty pageants and modeling scenarios catering to the general public have looks at odds with the preferences of most people, then attempting to do something about it, which is what this site is doing, cannot be critiqued by saying that beauty lies in the eyes of the beholder.
References
- Neel, J. V., Diabetes mellitus: a ‘thrifty' genotype rendered detrimental by ‘progress’?, Am J Hum Genet, 14, 353 (1962).
- Hauner, H., Rohrig, K., and Siffert, W., Effects of the G-protein beta3 subunit 825T allele on adipogenesis and lipolysis in cultured human preadipocytes and adipocytes, Horm Metab Res, 34, 475 (2002).
- Siffert, W., Forster, P., Jockel, K. H., Mvere, D. A., Brinkmann, B., Naber, C., Crookes, R., Du, P. H. A., Epplen, J. T., Fridey, J., Freedman, B. I., Muller, N., Stolke, D., Sharma, A. M., Al Moutaery, K., Grosse-Wilde, H., Buerbaum, B., Ehrlich, T., Ahmad, H. R., Horsthemke, B., Du Toit, E. D., Tiilikainen, A., Ge, J., Wang, Y., Rosskopf, D., and et al., Worldwide ethnic distribution of the G protein beta3 subunit 825T allele and its association with obesity in Caucasian, Chinese, and Black African individuals, J Am Soc Nephrol, 10, 1921 (1999).
- Siffert, W., Rosskopf, D., and Erbel, R., [Genetic polymorphism of the G-protein beta3 subunit, obesity and essential hypertension], Herz, 25, 26 (2000).
- Burt, V. L., Whelton, P., Roccella, E. J., Brown, C., Cutler, J. A., Higgins, M., Horan, M. J., and Labarthe, D., Prevalence of hypertension in the US adult population. Results from the Third National Health and Nutrition Examination Survey, 1988-1991, Hypertension, 25, 305 (1995).
- Cooper, R. S., Rotimi, C. N., Kaufman, J. S., Owoaje, E. E., Fraser, H., Forrester, T., Wilks, R., Riste, L. K., and Cruickshank, J. K., Prevalence of NIDDM among populations of the African diaspora, Diabetes Care, 20, 343 (1997).
- O'Dea, K., Cardiovascular disease risk factors in Australian aborigines, Clin Exp Pharmacol Physiol, 18, 85 (1991).
- Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: the evidence report, National Institutes of Health, National Heart, Lung, and Blood Institute, pp. 127 (June 1998).
- Sobal, J., and Stunkard, A. J., Socioeconomic status and obesity: a review of the literature, Psychol Bull, 105, 260 (1989).
- Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: the evidence report, National Institutes of Health, National Heart, Lung, and Blood Institute, pp. 22 (June 1998).
- Stunkard, A. J., Socioeconomic status and obesity, Ciba Found Symp, 201, 174 (1996).
- Seidell, J. C., Verschuren, W. M., and Kromhout, D., Prevalence and trends of obesity in The Netherlands 1987-1991, Int J Obes Relat Metab Disord, 19, 924 (1995).
- Lahmann, P. H., Lissner, L., Gullberg, B., and Berglund, G., Differences in body fat and central adiposity between Swedes and European immigrants: the Malmo Diet and Cancer Study, Obes Res, 8, 620 (2000).
- Lahti-Koski, M., Pietinen, P., Mannisto, S., and Vartiainen, E., Trends in waist-to-hip ratio and its determinants in adults in Finland from 1987 to 1997, Am J Clin Nutr, 72, 1436 (2000).
- Pietinen, P., Vartiainen, E., and Mannisto, S., Trends in body mass index and obesity among adults in Finland from 1972 to 1992, Int J Obes Relat Metab Disord, 20, 114 (1996).
Comments
although skinniness is what you refer to as "socially unacceptable", then why is that the majority of both men and women find thinness attractive? women are almost always striving to become thin and men almost always prefer thin women over average to overweight women.
i'm not talking about skinny as in anorexic, third-world starvation skinny, but skinny as in thin but healthy. i find it hard to believe that society doesn't find skinny models i.e. alessandra ambrosio or gisele bunchden acceptable. in fact, they are praised and envied because of their size.
Madeline: Skinny as in “thin and healthy” is not what I have described as something considered socially unacceptable by most people in Western societies. Read the entry linked to; the typical skinniness of high-fashion models is what is considered socially unacceptable by most people in Western societies. It is true that between slender/slim and overweight women, Western men generally prefer the slim ones, but slim here is much fleshier than the typically anorexic-looking high-fashion model.
As far as the likes of Gisele and Alessandra being praised goes, this praise is coming from the fashion industry, which shouldn’t be surprising, but these women are envied by few. Get women to go through pages within this site where the physiques of Gisele and Alessandra are addressed, and it is a guarantee that fewer still will remain in envy of their looks.
your site is poorly written; you tend to restate yourself over and over, and throw around terms like "transexual" and "gay" in order to bully your bluecollar audience into agreeing with you. Nice try overall! I would leave the site as it is and stop bothering with updates if I were you though.
ps: I'm very feminine, and I think the porno pix are hot, so don't even start.
Philomela: What does your comment have to do with this article? Since various commentators bring up the same issues, I have no choice but to repeat some points. This entry is aimed toward avoiding having to repeat -- in other threads -- the same comments about various correlates of beauty; all I have to do is to point the reader to this entry.
I don't see how blue collar workers will be "bullied" into agreeing with me based on words like "transsexual" and "gay." Why should I stop updating this site? There is so much more to add that I will never run out of materials. Besides, none of the pictures posted at this site qualify as "porno pix."
You haven't proven that extreme body modification is the result of the influence of psychotic shamans. You have created a hypothesis from scanty evidence. Please don't try to explain why groups you know very little about behave the way they do.
If significant groups of people have very different physical preferences from your average european then how does that fail to undermine "broad agreemant about what constitutes beauty"? The study you cited to prove that men and women prefer "above average feminiity in women" did not include the opinions of non-whites and non-asians.
If significant portions of non-white groups do indeed have different "intrinsic beauty standards" from europeans then shouldn't their ideals be showcased in international beauty competitions along with the standards of europeans?
If most people agree on "beauty" how come most people find your examples butt-uhglee?
I understand how some people, or even most people as u claim, find models unappealing or unimpressive,leaning to a more "feminized"look, but to claim most people find them ,or should find them masculine, to an extent of even calling them transexuals is ridiculous and exagerated.There is no need for such exageration ,its juvenile and unnecesary.Very few people would find the likes of Alessandra Ambrossio or Adrina Lima ugly or masculine ,unnapealing? indiferent? yes ,maybe , but ugly? transexual? nah! u know thats not the case.
BTW why would designers select models that remind them of the adolescent boys theyre sexualy atracted to(acording to you,obviously sugesting pedophilia)instead of selecting these women because thats what they wished they looked like if they were females? the latter makes much more sense. Has it ever passed your mind that these designers are not after all atracted to "adolescent boys" sexualy? and rather that they would want to look like adolescent boys themselves?
Im gay , and im not sexualy atracted to high fashion models because they look like boys...im attracted by them eastheticaly because thats what i wished I looked like if I was a female. OF COURSE gay men would rather look tall,thin and aloof , rather than busty,with wide hips and plain faces. DUH. Your sugestions of pedophilia make no sense,thats all on your head...you got issues.
forgot to "sign" the above message.
Danielle: What do you mean by the following?
Quote:
Maybe you meant to write that it does undermine the argument. The major correlates of beauty apply across cultures. The literature review I cited about people’s preferences for femininity included studies that have used European, Japanese, Chinese and other groups. Here is an additional study that had Jamaican samples (predominantly sub-Saharan African) and also reported a preference for above average femininity in women’s faces:
Quote:
In this study, Jamaican males preferred less feminine exaggeration in women (white, Japanese, Jamaican) than British males, but the authors mentioned a confound in the form of Jamaican men preferring more feminine exaggeration for Jamaican women than for white women, but then sub-Saharan African women generally don’t have faces that look that feminine to start with.
I have no problems with major geographic populations using their own standards in international beauty pageants since I have proposed splitting these contests along the lines of broad ethnic groups and the winners from each group competing with each other in a personality contest. This avoids the problem of objectively comparing the attractiveness of women from different ethnic groups, something that cannot be done.
If you are not convinced about influential shamans being behind bizarre painful rituals, I suggest that you start with the following paper:
Quote:
In this paper, Michael Persinger cites evidence relating some brain abnormalities behind temporal lobe epilepsy (TLE) or partial-TLE symptoms that result in god beliefs and by virtue of anatomical location are undoubtedly associated with brain abnormalities related to sadomasochism, a broad spectrum of sexual disorders and a violent orientation. Shamans are notoriously often epileptic or psychotic. This would explain, among other things, why religions throughout history have been full of sadistic rituals and why the notion of salvation through pain/suffering/sacrifice has been common, and also why the zeal and fervor with which people have carried out God’s work in the form of mass murder is generally not matched by mass murder motivated by non-religious causes. Persinger and others have since authored many papers. Whereas these papers are not written for laypersons, Persinger has written a book for the general public, Neuropsychological Bases of God Beliefs, which I recommend you read.
After reading the evidence, ask yourself why would people mass-adopt painful crazy rituals when people are generally inclined to avoid pain?
Adrian: What do you mean most people find my examples of feminine beauty butt-ugly? The vast majority of people that have gone through this site have not left any comments, let alone addressed this issue. Then, there are angered homosexuals/masculinized women/feminists who have left comments in opposition and have a stronger motive to leave comments.
I haven’t been calling models transsexuals, just pointing out that a number of fashion models have the looks of male-to-female transsexuals. Alessandra Ambrosio is an obvious example, and I have never said that Adriana Lima has a transsexual look. I haven’t described fashion models as ugly.
As a general rule, men who fantasize about looking like women wish to look feminine, not like the norm among high-fashion models. In addition, it would be difficult to find men who want to look like adolescent boys. The most obvious explanation of fashion models’ looks is obvious. Much higher rates of sexual interest in underage individuals among homosexuals and bisexuals is not just in my head, but backed by a tremendous amount of evidence from history and the present.
Adrian, thank you!:
Adrian wrote:
Quote:
I am a straight woman and I have always believed that gay male fashion designers choose female models as projections of their own fantasy female selves.
I knew that if I expressed this belief on this website I would lack credibility as a straight woman claiming to speak for gay men, so it is nice to have a confirmation by a gay man who is qualified to speak for gay men.
Erik's belief that gay male fashion designers are attracted to teenaged boys even if they NEVER have sex with teenaged boys is irrational. Most successful gay male designers live in places where the age of consent is 16 or lower and they choose to say no to legal, easily available sex with teenaged boys because they are not attracted to teenaged boys.
:blank:
Whipped Honey,
Gay men often "suffer" the "peter pan syndrome"(wanting to be young and "pretty" forever),therefore I believe gay designers preffer models who have childlike traits(thinness,age).Im almost sure its not because they are attracted sexualy to underage boys.
Most gay men are attracted to men who are masculine or hyper masculine,who posses an agressive nature(in other words ,the "straighter" the better),its unlikely that they are attracted to fragile little boys(that the current high fashion models ressemble).
Lets be honest here, most gay fashion designers are most likely bottoms sexually,I doubt they have fantasies of abusing fragile little boys...rather than wanting to be abussed themselves! lol
Gay designers are very open about their sexuality, and tho I cant sustain it with reasearch,I doubt that child molesting homosexuals are openly gay or have the tipically femenine interests of the very openly gay designers.I repeat ,tho I cant sustain it with any type of research(there must be research of this type in existence)the tipical profile of the homosexual pedophile is a man who is not openly gay ,and married.I cannot present any proof, but pedophiles are most likely indiferent to the gender of their victims, pedophiles most often abuse boys as well as girls,since their gratification lies on the victimization/domination of their subjects,not their genitals.
Of course there must be pedophiles who are exclusively interested in boys,but I dont think thats very common among them.
Erik wrote:
"I would be difficult to find men who want to look like adolescent boys"
true...youre talking about straight men, or average gay males(who do not work in the fashion industy,with a lifestyle ranging from closeted to "straight-acting").
But believe me,it wouldnt be very difficult to find gay men in the fashion or beauty industry that would like to look like an adolescent boy, for many reassons...
main ones:
looking like models(models ressemble adolescent afterall boys dont they?)
looking "good" in any type of clothes(the type of clothes openly gay men ,especially fashion designers like to wear)
having bigger chances of attracting a masculine man ,or the ellusive "straight guy" (the holy grail for gay males)
Erik,
I think Adrian has a point here: Gay designers prefer young and masculine looking models not because they are latent pedophiles, but because they (subconsiously) pick the petit and masculine women who they adore and would want to ressemble, IF they were a woman.
Paul.
P.S. This is not the best English I ever typed, I know :)
Whipped wrote:
That refutes a minor, if irritating, but unecessary point of Eric's, but tends to confirm rather than refute his larger points - That gay designers dominate the fashion industry and choose models based on their own personal aesthetics, rather than the aesthetics of the wider population. The fact that they're disproportionately choosing sickly-thin women with boyish faces and then putting makeup on them that often makes them look like they were dragged out of a local crackhouse right before the show because that's what they fantasize about looking like themselves doesn't mean that's what the majority of the public finds attractive.But really whether they do it for that reason - their fantasy-self is a emaciated crack addict with a boyish face - rather than because they fantasize about having sex with emaciated adolescent boys strung out on crack - has little to do with whether that's what the general public fantasizes about.
For what the average red-blooded male fantasizes about, it might be better to look at comic book superheroines - admittedly a very fantastic (unrealistic) portrayal, but the vast majority of superheroines (drawn largely by hetro males and for an audience disproportionately hetro male) look nothing like the typical runway "high fashion" stick-figure (who have figures just as "fantastic"/unrealistic for most women, unless they literally starve themselves to near death).
Cut it out from your head whom said gay male choose fashion women from their fantasy female selves.
The fashion started first time by " COCO CHANEL" she was the most unique girl of that time. while the other women was still struggle in the ideal of ancient beauty that the pretty women had "S" shape ( like Erik said) blond hair and what ever... Chanel had changed all of this by accidentally. she was a girl from low class family from southern europe. with the skinny body shape because of poor family. she had not much time to bussy with a long swoll hair like the high class woman in that time were. so chanel let cut her hair and designed the dress and cloths in lovely style to suit for the active working little woman like her. it was strange for the guy like erik. seem a lot of high class males in that time even the royal families, like the woman like chanel and there were a lot of high class males fell in love with her. in her character and her looking. she turned to be very famous and all untill the pale plump woman in "S" shape jealous in her lovely and cute. so they tried to copy the character, the cloths and looking of chanel. that was the history where the skinny women begin and I think everyone on here also think the same that the cloths are more prettier when on the skinny little women.
Anyone who knows anything about evolution knows that beauty is in no way in the 'eye of the beholder' otherwise Angelina Jolie and David Beckham are in one hell of alot of beholders eyes....
Since humans ARE animals, you'll see the same effects in other animals, not just humans. A famous example of this is a research paper entitled 'Female choice selects for male sexual tail ornaments in the monogamous swallow' by andreas moller.
Beauty is in the eye of beholder !
and lastly,evolution is not a fact.
God created humans.
Do you think Lee Hyori South Korean Pop singer -beautiful ??
Here's few Hyolee pics.
http://www.zr5.net/wp-content/uploads/2007/12/sexy-lee-hyori-2.jpg
http://img248.imageshack.us/img248/4424/leehyoriva01tv2.jpg
http://hyori.net/20040130_LA/photo_008_202.jpg
http://hyori.net/20040130_LA/photo_008_212.jpg
http://img372.imageshack.us/img372/2461/200702071924042030nn4.jpg
http://s2.supload.com/files/default/hb1195722546_Image_0782.jpg
Many South Korean man love her and deem her as attractive woman ,and no they aren't gay ,bi or etc .
If i think she's pretty,than i must be sick or abnormal to you ??
I am not Asian by the way.I am from NY =originally from Russia.
I find Asian women just as beautiful as White ones.
I am curious ,are you Nordic North European ??
Erik : what do you think of kathrina kaif, the indian part english?
I think she looks gorgeous like greek's goddess, all of her facial's features are porportion, big set beautifull eyes.
Last one of katrina kaif.
I like this two picture of katrina but since she getting older it seems like her shape begin to get more buxum, thick shoulders and waist like latino women.




Also if you look closer you'll find it is the same features of a skull and face that are consistently being the cause of attractiveness, e.g. large, wide set eyes in women, broad forhead in males etc. Just more evidence for the fact that beauty is universal and not in the eye of the beholder.
Many pschology journel publications have papers showing this.
zonneschijn, that lady looks like a horse.
hannah : you see? beauty lie in the eye of the beholder. I put the pictures of katrina kaif. the Indian part British supermodel on here because I find she has the weak jaw and weak cheeksbone, big breasts and wide hip following the " beauty's cristeria" of erik. some people like you may find her face looks like a horse because the jaw and cheeksbone are very weak? so what's the true beauty then if it dosen't lie in the eye of the beholder?
some woman got epicanthic fold then you find she has
disportionate eyes?
some women got sucken eyes you find she got eyes like men?
some women got big set eyes, you find she got eyes like black people?
some women got double eyelids you find she looks old?
Katrina Kaif, beautifull Indian/British supermodel/actress of India.

What do you think about katrina kaif's back, erik?




Oh my !!
Your half English/Indian model is hott and nice looking !!
Yes, she looks very gorgeous on India flims.
Everyone try to find this flim to watch, katrina is very gorgeous.



I feel I should give this link:
www.lookism.info
Its alright to define exactly what beauty is in a biological sense, but don't go and discriminate against those who don't match exactly as what society deems attractive -
looks are not earn't, but handed on a plate by DNA.
Erik, if northern europeans have historically had the most intense sexual selection...
What about in modern times with contraception?
In Western Culture a lot of men have a huge number of sex partners and don't comitt till much later in life.
Attractive women get used and tossed out, not getting a chance to fulfill their ambition to have kids.
I have seen many attractive women in the 30's who have not found 'The one', that is because contraception has allowed their potential husbands to sleep around and these men fulfill this desire. Contraception skews the natural balance of partnering and reproduction.
'Attractive' men no longer want to settle down, they want to 'have fun' and screw women around and contraception gives them the power. If contraception is abolished then you will see that attractive women start marrying more and having more kids.
The myth that casual sex is 'liberating' for women and an 'equal opportunity pleasure' for women, needs to be stamped out.
In Australia, the birth rate is at 1.7 babies per woman, I have seen no evidence that attractive women have more babies.
In fact there really isn't a lot of dating in teens and adolescence, even in a woman's 20's.
These days there are more hookup's and fuckbuddies. Marriage rates and comitted relationships continue to decline. A lot of children tend to come out of marriages. However, if you are a university educated female, as I am, your chances of every marrying are already a lot lower than woman who have no university education :S
Erik, as for the effect of globalization and mass migration on various native populations, have you seen the following website?
http://www.faceoftomorrow.com/
It's interesting how the face of Bondi, Sydney turns out a lot more British looking than the face of London, England!
A picture of an Ainu women with tattooed mustache might be a worthwhile addition to the body modification gallery.
On the matter of shamans (applicable to religion generally) tribes are in conflict with one another and if the shaman derived tribal practices differ then the most disadvantagous practices will tend to be removed by natural selection. So many shaman might have been mad and got their tribe to do something very stupid which could become a tradition, but it couldn't be too stupid if they survived. No doubt many tribes have disappeared because they did believe in the shaman (and tribal deity) and the shaman told them not to take violent bloody actions against their neighbouring tribe or the shaman prophesied that the neighbours were going to become too strong for them that the time pre-empt their attack was now, but the tribe said we don't beleive you or thought war was too risky
The enforcement of public morality has great advantages in this group selection so a shaman might be suggesting something really stupid but if it caught on it might have something going for it, for reasons that never entered his head probably. Lets take circumcision as an example, a form of body modification that has been promoted (since ww2 for some reason) as healthy. Now a new wave of promotion is being launched it is supposed to partially protect against HIV This, along with the the strict Muslim beliefs on sex, is said to account for the low rate of HIV in Senegal. So the body modification of a long standing religion is a positive boon to a peeople who practice it.
Or maybe not, maybe the men of Senegal have something else going for them that affects HIV according to James Mackintosh ( Mackintosh,J,A,.2001 'The Antimicrobal Properties of Melanocytes Melanosomes and Melanin and the Evovlution of Black Skin' Journal Of Theoretical Biology 211:101-113) it's all down to the colour of their skin, foreskin mainly, which needs to be resistant to infection because their high T. levels depress their immunity.
What Erik is trying to convey is how many beholders, but it might be too late to change the title into "In the eyes of how many beholders does your beauty lie?" Just run your own pageants and your own magazines if you want to do more than having this site up and promoting whatever other Web sites you like. In the U.S., even though people don't want looks to run their lives, they wouldn't do anything to you as long as you don't deceive them (hint: drop all the sketchy arguments) or threaten their basic freedoms.
Been looking for this post. While the idea of some of these traits being cases of exagerated sexual dimorphism are valid, some of them most certainly aren't- for example, head binding, which results in a low, sloping forehead that Erik treats as instrinsically masculine.
Plus, just how many of these practices are the results of shaman forcing them on people? The burden of proof is on Erik for this one.
Totally agree with you, Dingelberry, you seem one of the few ppl that actually got the point of this site!
Erik,
You made this comment in the article:
"Masculine looks in women are disproportionately preferred by homosexual/bisexual men, lesbian/bisexual women, women with gender identity disorder, anorexics, bulimics and masculinized women (anorexic and bulimic women tend to be more masculine than normal women, on average; see evidence from sex hormone profiles). "
Can you please provide articles and/or statistical data backing this up? I've always had a theory that the grand majority and the most vocal supports of fashion industry female models are gay men (naturally) and women that are not well endowed and/or curvy. When I bring this up I am almost always attacked for supposedly being homophobic or completely crazy.
This also leads me to another matter. While in this article you make an argument that social conditioning isn't the only factor I really do think that you need to address in a new article the social conditioning that has occurred due to the iron grip that the fashion industry has taken on the mainstream industry that has resulted in pretty much every women in show business being made to be as thin as they can be and to downplay any curves they have.
I'm not not talking about women falling into eating disorders because of pressures but specifically speaking how most people who talk about women have the mental image of really thin women with little to no curves being supposedly the best kind of body type a women can have.
While I understand and agree that many of these people tend to be gay men, I still don't see at least an equal amount of straight men arguing otherwise. In fact, it seems to be that most white males regardless of their sexuality currently prefer thin women with little curves as possible and will easily call any women who doesn't fit into that mold "fat". Just look how quickly female celebrities who don't look stick thin will be called "fat" at the drop of a hat by TV and radio hosts, internet websites/blogs, etc... and there is little opposition heard in any kind of forum.
What I am asking is that while you may provide statistics that say one thing, in society this does not appear to be reflected by the public, specifically speaking white men.
I believe that the fashion industry hold on mainstream media has created a social conditioning that has made many in the public internalize their female beauty standards that might have otherwise not have agreed to such. Some, such as myself, have not been affected but I believe others have been.
I would appreciate your thoughts on this as well as considering a future article discussing the possible social conditioning that the fashion industry's influence has created.
I agree with you, Jim, and I think that many hetro men are getting obsessed with the image that a bit too thin is better than normal, and most ppl don't realize they're affected. I think it started because the hollywood actresses became affected by the models, and I've read several articles online where mainstream actresses speak out how they were pressured to lose weight for hollywood movies, and very few have stood up to it and refused like Kate Winslet who talks about it online& has taken a stand against it. However many women have given in to the overly skinny and unhealthy look like Calista Flockhart from Ally Mcbeal show who always looked scary thin and sickly, she recently admitted to an eating disorder.
So the problem is that the mainstream hollywood actresses- pressrized by hollywood producers- have copied the fashion modeld and tried to lose too much weight (not as much as models but too much to be healthy) and the problem is that regular young women from the general public are interested in copying and emulating the looks of actresses , so it becomes a problem for many ppl
i.e.
actresses are affected negatively by models to lose weight
then normal women are affected by the actresses to lose too much weight
So it becomes a vicious cycle
Here are a few articles to illustrate my point, all talking about the weight issue of hollywood actresses losing too much weight and sending a negative message to women
We can all agree I think that actresses are influenced by models and that many women are influenced by the actresses if not as much the models
But obviously the result is the same - bad- for obvious reasons
So I hope I explained your point , Jim, as I agree with it and was also thinking that Eric needs to address it as some point
Here are the links to the articles mentioned:
search.hollywood.com/movies/Skinny%20Actresses
www.dietingdelilah.com/most-scary-thin-celebrities/
www.geocities.com/hollywood/4616/ppl1018.html
www.hilary.com/fashion/bikini.html
www.sodahead.com/...hollywood...actresses...too-ski...
And check this one out very interesting
THE UNWRITTEN WEIGHT RULES FOR HOLLYWOOD ACTRESSES
www.ivillage.com/...hollywood-actresses/4-a-21452...
And the best of all: the article that shows WHAT HOLLYWOOD ACTRESSES REALLY DO TO LOSE WEIGHT AND WHAT DRUGS THEY TAKE LIKE ADDARELL and drinking coffee, smoking all day, and laxatives
Here's the dirt
http://www.wellsphere.com/weight-loss-article/how-celebrities-stay-so-skinny/6731
Article on the amount of hollywood actresses speaking out about having anorexia/ bulimia/ eating disorders:
http://www.edreferral.com/Celebrities_who_died_or_have_Eating_Disorders.htm
Jim: Regarding evidence for masculine looks in women being disproportionately preferred by “homosexual/bisexual men, lesbian/bisexual women, women with gender identity disorder, anorexics, bulimics and masculinized women,” this is an inference I have drawn.
If you look at representative surveys of sexual interests and behaviors, among those that have either voluntarily indulged in homosexual behavior or experienced same-sex attraction at some point in their lifetimes, very few, including a small proportion of self-identified gays and lesbians, have neither voluntarily engaged in heterosexual sex nor experienced opposite-sex attraction in their lifetimes. You can find some old evidence for it here (newer surveys show the same thing): http://www.homosexinfo.org/Sexuality/Variability and http://www.homosexinfo.org/Origin/Support
By extrapolation, the appeal of masculinized women will be greater for the nonheterosexual group because such women are in between male and female average looks.
One can observe a higher prevalence of nonheterosexuality among those with gender identity issues: http://www.homosexinfo.org/Psychiatry/Transgenderism
Correspondingly, the appeal of masculinized women will be greater for the group with gender identity issues.
Mentioning the cited evidence will not help you avoid accusations of homophobia.
Evidence that the sex hormone profiles of anorexic and bulimic women tend to be less feminine has been cited already, which should correspond to a less feminine appearance on average, and it is known that a number of them are influenced by less feminine, on average, high-fashion models, suggesting greater salience of masculinized women to such women [this is a weak contention, and even I would not bet on it].
You have also asked me to explain “the social conditioning that has occurred due to the iron grip that the fashion industry has taken on the mainstream industry that has resulted in pretty much every women in show business being made to be as thin as they can be and to downplay any curves they have.” But this is not an instance of social conditioning.
When you mention show business, top publications, TV and Radio, the choices are made by few people notwithstanding a superficial diversity of TV stations, magazines and people, and the choices do not necessarily reflect the preferences of the general public. You need to look at controlled studies, and it becomes very clear that the majority in Western nations optimally prefers, in women, a subset of the medically normal body weight range and above average femininity.
If you do not understand the discordance, ask yourself what are the odds of me writing for a major mainstream magazine or newspaper or perhaps be involved in a position of prominence related to what is disseminated via TV or Radio? Nil, not because I have nothing useful or interesting to say or because I cannot back up my arguments with evidence, but because some people have spent much time and resources on effecting social change and maintaining certain positions that someone like me may undermine. These people will be vary of personalities who show independent and critical thinking skills, even if such thinkers have not yet written or said something that displeases them. Correspondingly, do not confuse the banal, the mundane, the garbage and the relative homogeneity coming from the top as evidence of social conditioning or widespread endorsement. Controlled studies show a very different picture, and not just about beauty preferences, but also about political attitudes and other things that matter.
True beauty is universal and transcends race or species.
What humans consider beautiful in birds and animals seems to be appreciated across the species.
A beautiful male bird of paradise is not only enjoyed by Attenborough but also by the female of the species and rest of the world.
Satyam Sivam Sundaram.
Thatwamasi